ADVANCED KERATOCONUS TREATMENT WITH PHORCIDES
Keratoconus treatment is based around stopping progression and improving vision.
Corneal collagen cross linking stabilises keratoconus but usually does not have a great effect on the corneal irregularities that reduce the quality of vision.
Combination of excimer laser topographic phototherapeutic keratectomy at the same time as cross linking has the opportunity to reduce corneal irregularity and improve vision at the same time as stabilising the disease. The analogy is that in keratoconus the eye is like wet concrete that is changing shape. The cross linking makes the concrete set, but the shape is still not normal. Laser sculpts the concrete at the same time.
THE PROBLEM
When an excimer laser is used to treat corneal irregularities, this will have an impact on the refraction. Up until now, there has not been a systematic method to analyse and predict the refractive effect of the complex shapes in a customised topographic ablation profile. Experts would make estimations based on the general shapes, positions and depths of the ablation profile and adjust the refraction that was to be treated. A variety of different systems have been described but often the end result was refractively unpredictable.
THE SOLUTION
The Phorcides Analytic Engine is a breakthrough technology that has the main function of predicting the refractive effect of topographic laser ablations. This is achieved by considering each significant area of the topographic ablation plan as a “talus”. Each talus is calculated as a vector that has both an angle and magnitude. These vectors are combined to give an overall sphere and cylinder effect of the ablation.
Phorcides does not stop there - it then takes into account the subjective refraction as well as the anterior and posterior corneal astigmatism from a tomography device to give a recommended overall spherical and cylinder correction.
The outcome is a much more scientific approach to the refractive analysis of topographic laser profiles and more predictable and repeatable results. Phorcides can give impressive results when applied to LASIK where it makes the good even better, but it is also extremely powerful in helping plan treatment of diseased corneas such as keratoconus.
AN EXAMPLE OF PHORCIDES IN ACTION
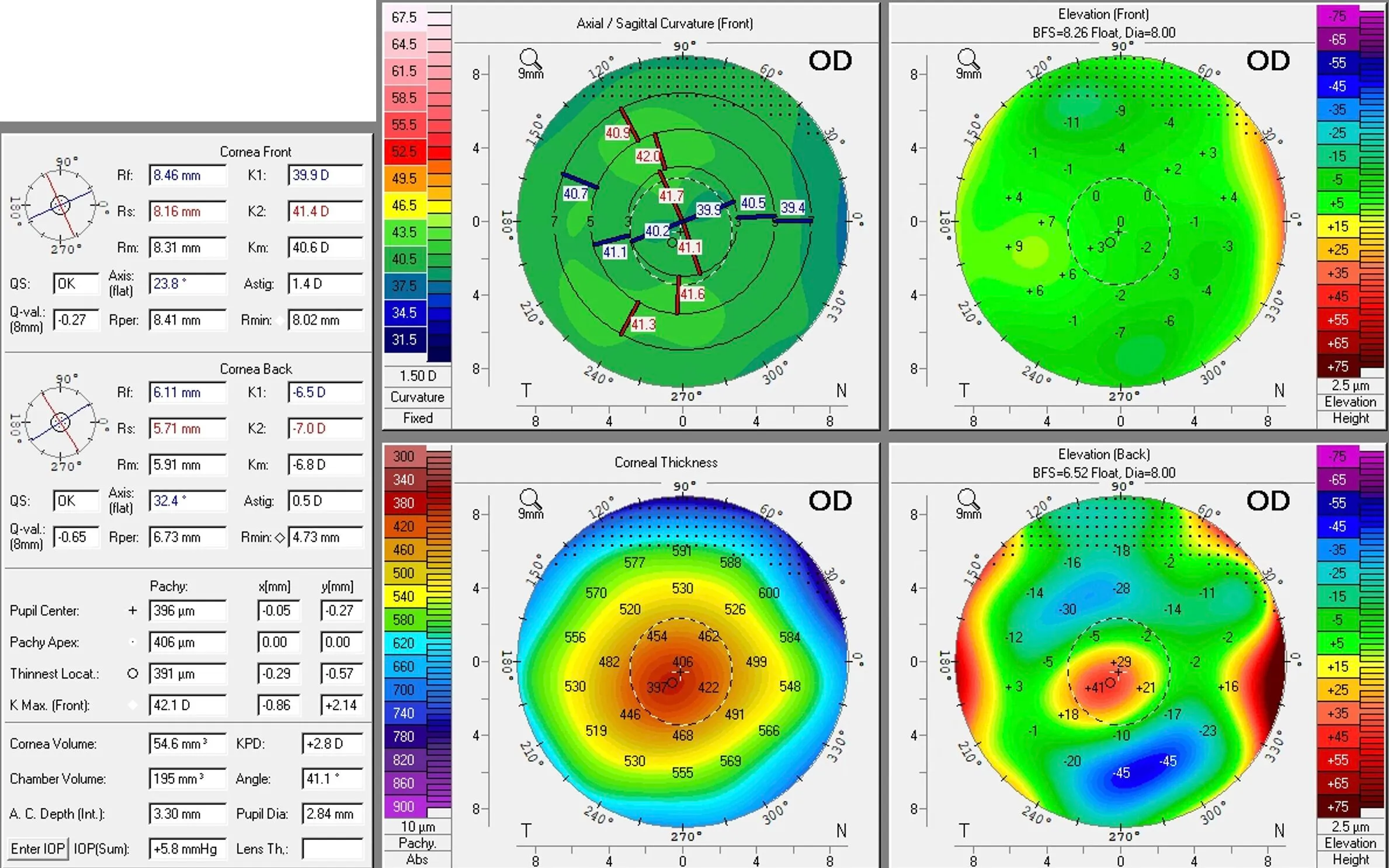
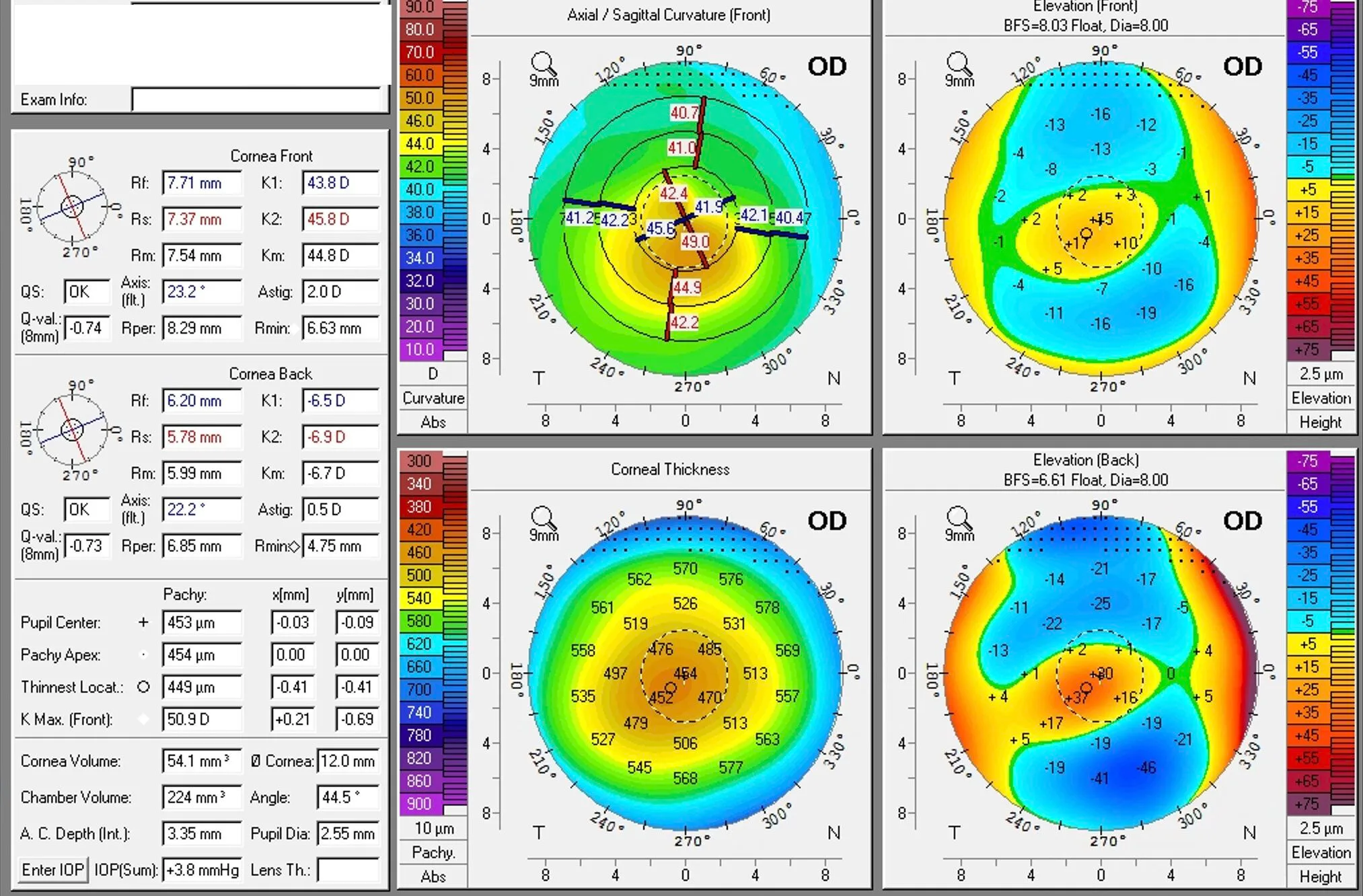 Preoperative tomography in keratoconus
A newly diagnosed keratoconus patient. Corrected visual acuity 6/15 with poor quality of vision.
Preoperative tomography in keratoconus
A newly diagnosed keratoconus patient. Corrected visual acuity 6/15 with poor quality of vision.
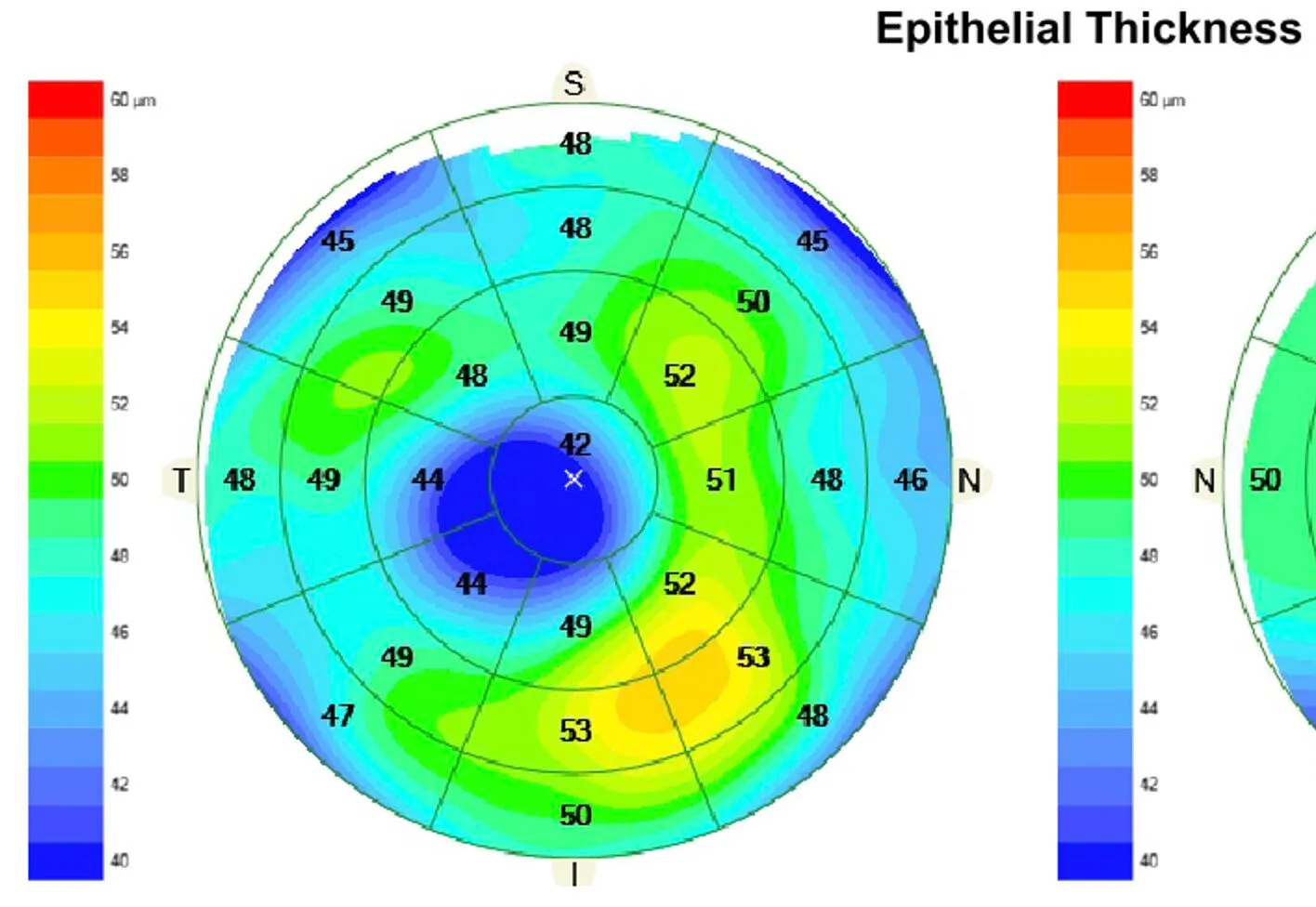 OCT epithelial thickness map
OCT epithelial thickness map showing epithelial thinning over the cone surrounded by a thickened annulus. This is a characteristic finding in keratoconus epithelial maps.
OCT epithelial thickness map
OCT epithelial thickness map showing epithelial thinning over the cone surrounded by a thickened annulus. This is a characteristic finding in keratoconus epithelial maps.
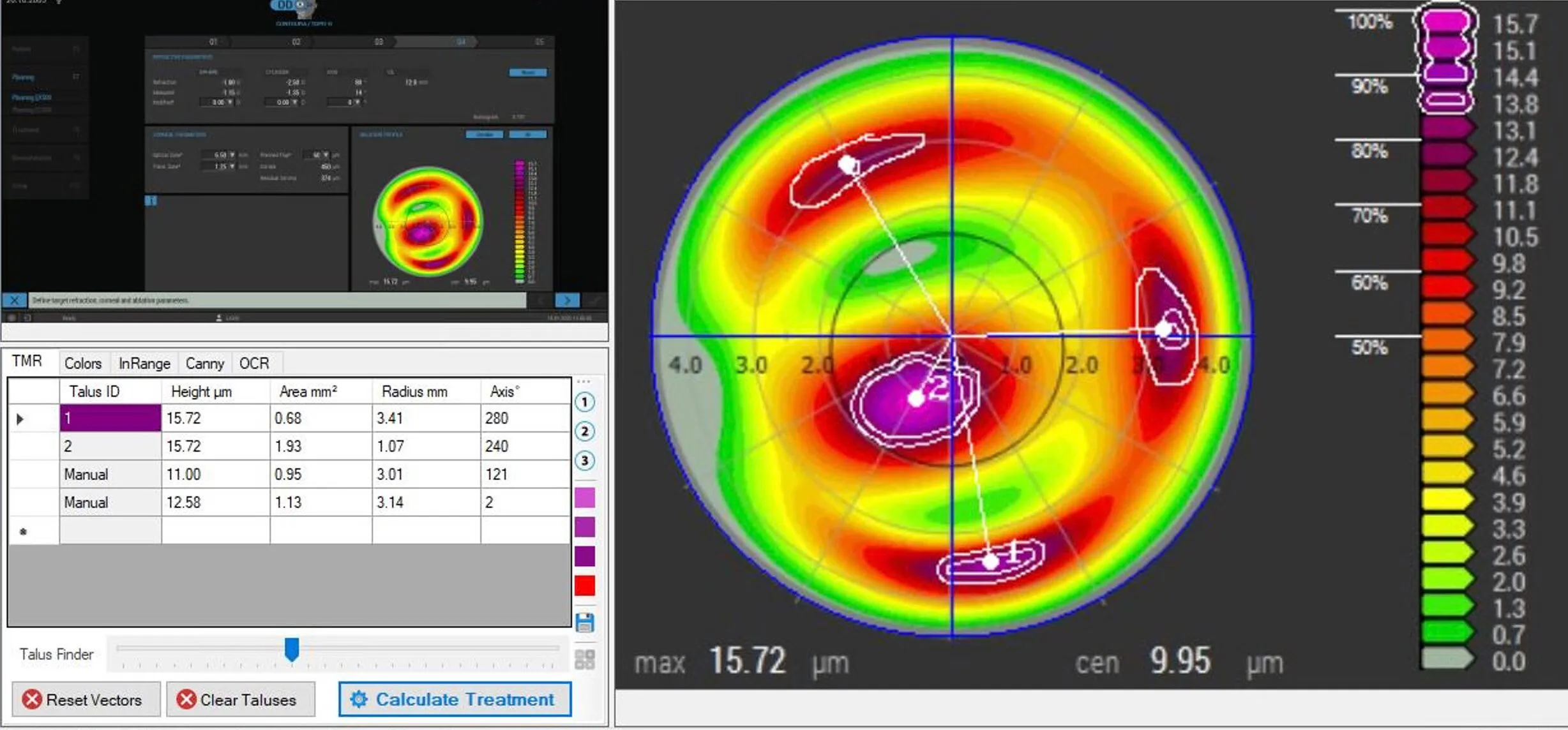 Topographic ablation profile on the Wavelight EX500 and Phorcides Talus Analysis
The ablation profile is planned on an Alcon EX500 Wavelight. The topographic laser treatment has been planned and all refractive components set to zero. This means that the ablation profile is purely to designed to deal with higher order aberration topographic abnormalities. The image is imported into Phorcides which has identified 4 significant taluses.
Topographic ablation profile on the Wavelight EX500 and Phorcides Talus Analysis
The ablation profile is planned on an Alcon EX500 Wavelight. The topographic laser treatment has been planned and all refractive components set to zero. This means that the ablation profile is purely to designed to deal with higher order aberration topographic abnormalities. The image is imported into Phorcides which has identified 4 significant taluses.
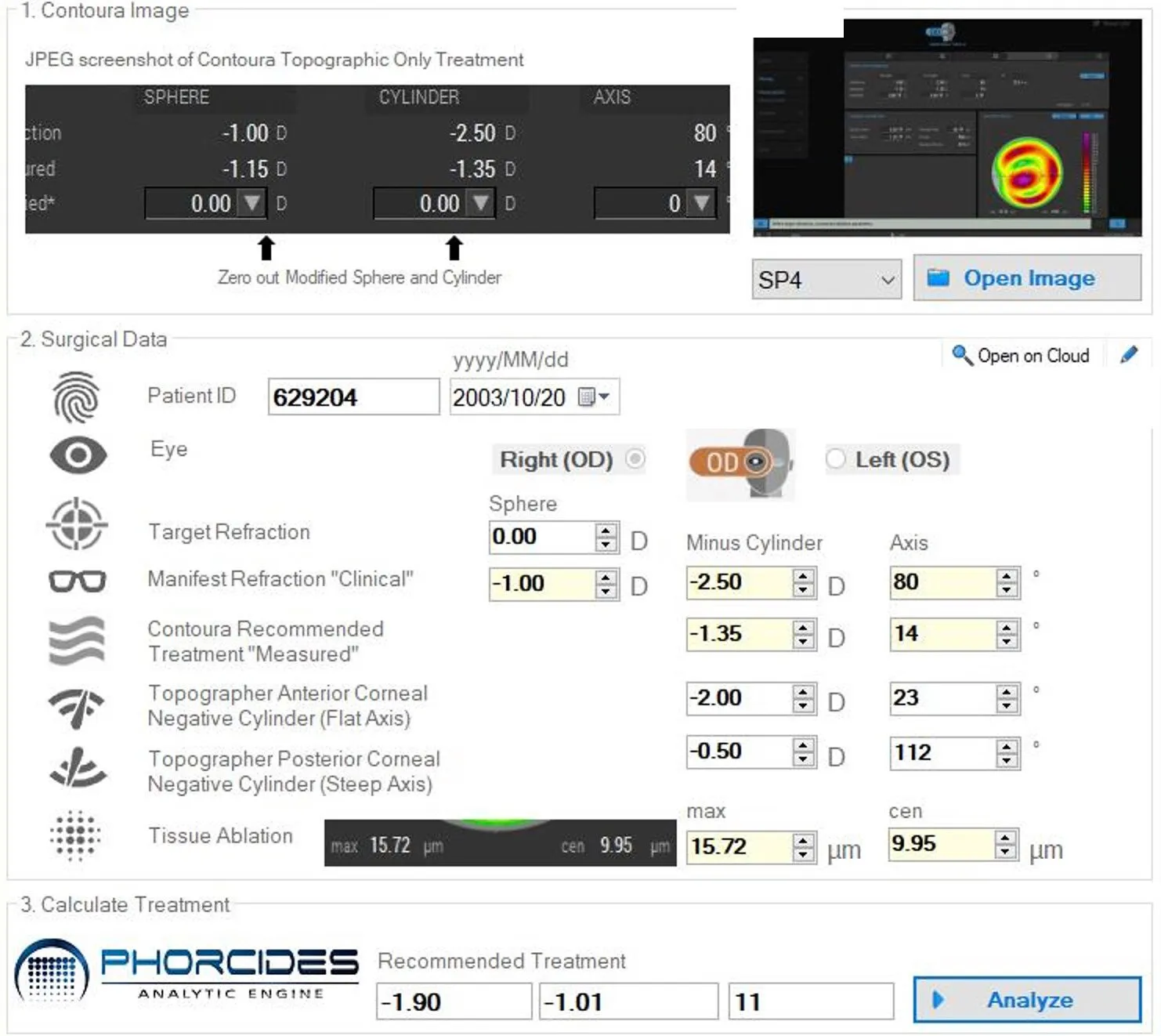 Phorcides Recommended Treatment Plan
Phorcides Recommended Treatment Plan
The patient wants 2.50 D of cylinder at 80 on their manifest refraction which disagrees very much with topographic cylinder. Phorcides calculates that in fact we should treat -1 D at 11 degrees. Phorcides also has an inbuilt EX500 nomogram so personalised nomogram adjustment is not required. The laser was performed in a transepithelial format in two parts -
- Contoura treatment of -1.65 / -1.01 x 11 onto the epithelium - under the patients name with her topolyser obtained data for cyclotorsion control. Max depth 44um
- A Streamlight treatment of -0.25 D at a 6.5mm treatment zone and minimum epithelial depth (45um) - under a dummy patient file to allow immediately sequential treatment. Total central depth 49um
My Reasoning for this methodology
-
Topographic data is taken from the epithelial surface which has irregular thickness. As soon as the epithelium is removed the front surface is different - transepithelial treatment makes sense.
-
Keeping nearly all of the refractive correction in the contoura component makes sense as the ablation profile is mixed and accounted for in the Phorcides nomogram. This is compared to the two step nature of the streamlight where an excellent transepithelial profile is followed by the traditional wavefront optimised profile where personal nomogram adjustments may be required.
-
Performing the topographic component first and directly onto the epithelium. This is when the cyclotorsion control is likely to work best; the patient is not yet fatigued and will likely have the best fixation before stromal ablation starts to blur their view.
-
A dummy patient is used as wavelight software prevents sequential preplanned treatments on the same patient and eye on the same day. It allows pre planning of the treatments, less than 60 seconds change over time and no new ablation profile planning is required on the fly.
-
The dummy patient is used for the transepithelial part of the ablation as it is rotationally symetrical so no cyclotorsion control is needed for this component.
-
Streamlight used instead of PTK as the transepithelial ablation profile inbuilt in streamlight is predictably refractively neutral.
-
0.25D of myopia moved from the contoura to the streamlight treatment to allow its use - streamlight can’t perform a 0 D ablation.
This was followed by MMC 0.02% for 20 seconds and then an accelerated epi off KXL cross linking protocol 7.2J at 9mm zone.
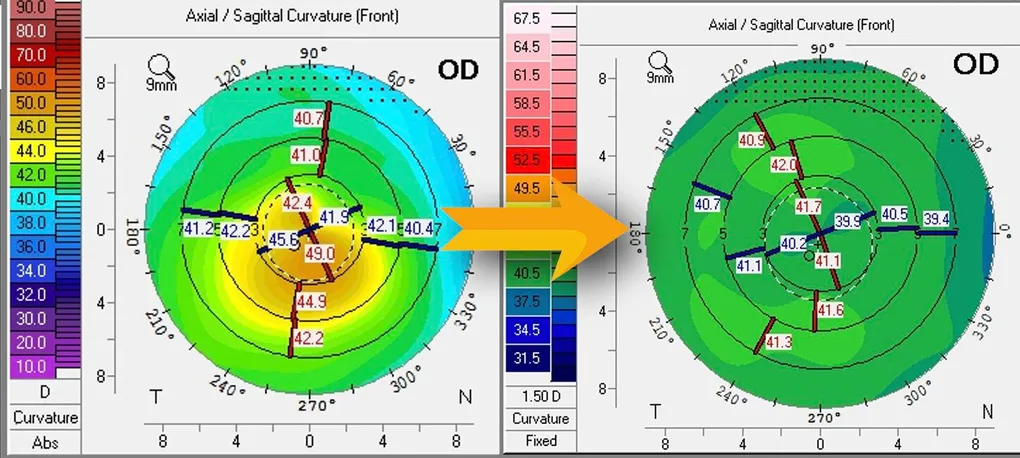
 Tomography 1 month after Phorcides guided topographic laser and cross linking.
Tomography 1 month after Phorcides guided topographic laser and cross linking.
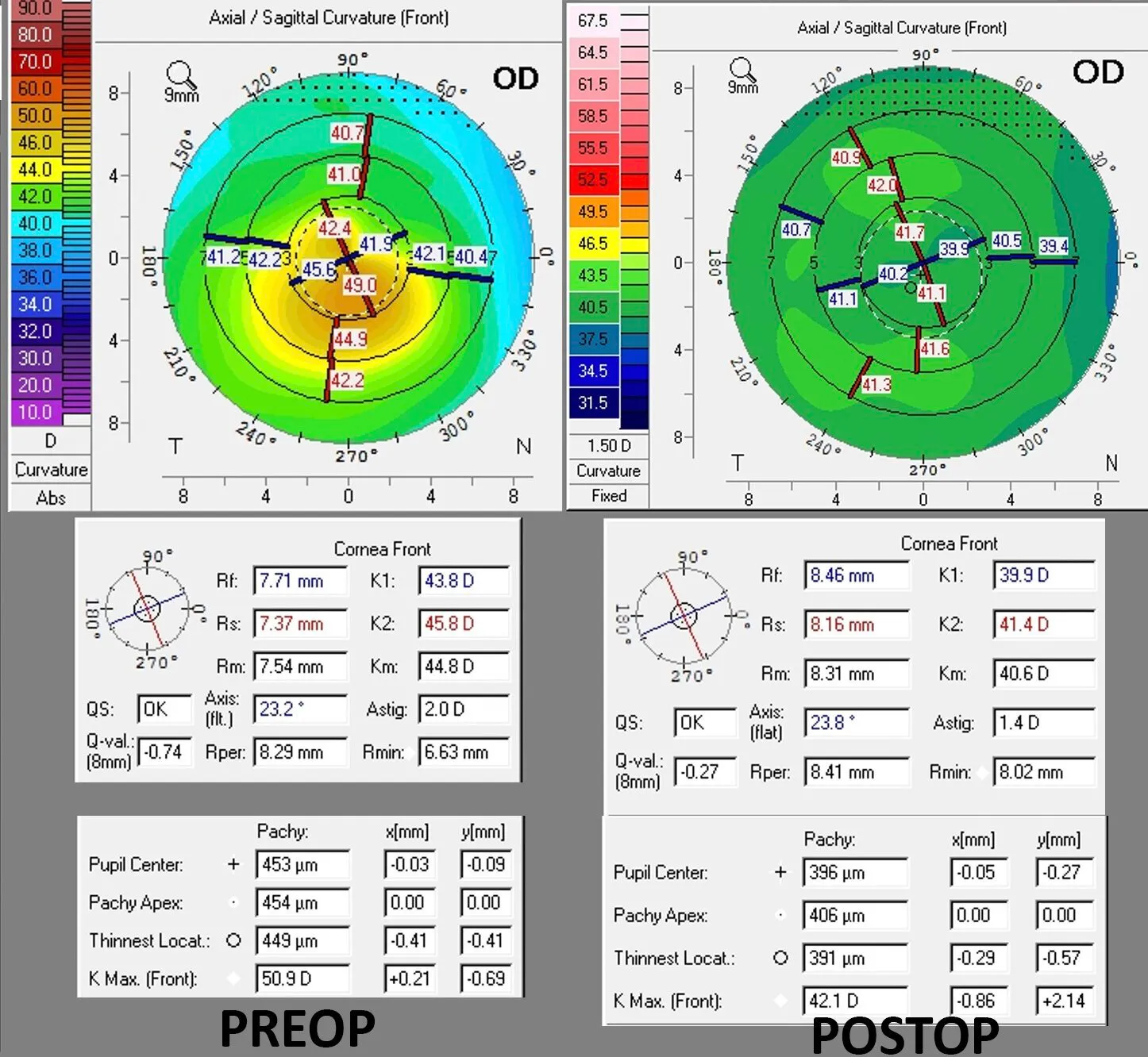 Before and After Surgery
The patient began with a CDVA of 6/15. 1 month after treatment she obtained 6/7.5 uncorrected with much improved visual quality (CDVA 6/6+ with 1D cyl). Kmax reduced from 50.9 D to 42.1 and corneal irregularity was much reduced. She was extremely happy and the vision is likely to improve further as the mild corneal haze from the cross linking improves. This is an exciting new treatment and as experience grows with the technology, things are likely to improve further.
Read more about Phorcides here.
Before and After Surgery
The patient began with a CDVA of 6/15. 1 month after treatment she obtained 6/7.5 uncorrected with much improved visual quality (CDVA 6/6+ with 1D cyl). Kmax reduced from 50.9 D to 42.1 and corneal irregularity was much reduced. She was extremely happy and the vision is likely to improve further as the mild corneal haze from the cross linking improves. This is an exciting new treatment and as experience grows with the technology, things are likely to improve further.
Read more about Phorcides here.
